Our portfolio of instruments, consumables and services are designed to help you maintain regulatory guidelines, ensure data integrity, and meet GMP requirements.
Our portfolio of instruments, consumables and services are designed to support clinical lab regulations, standards and with HIPAA data security in mind.
Liquid delivery is one of the most common processes in life science laboratories, from drug discovery and compound management laboratories to analytical chemistry and genomics/proteomics facilities.
These laboratories use liquid delivery for processes including sample preparation, dilution, standards preparation and reagent addition. However, the means for delivering liquid samples have advanced drastically over time, from the traditional glass micropipette to today’s electronic, variable volume pipettes and automated liquid handlers. Liquid delivery processes are further complicated by a radical reduction in the average volumes handled. Combining these trends with the potentially significant consequences of liquid delivery error, such as non-compliance, wasted time and money, inefficient use of scarce samples and compounds, and false data, it is clear that liquid delivery can be a major source of risk. Processes must be put in place to monitor, manage and minimize this risk, making the need for liquid delivery quality assurance (LDQA) urgent.
From improper operator technique to fluid viscosity issues, to variable environmental factors and internal pipette component damage, the sources of error are many and the potential for failure is real. Given the numerous factors that influence the accuracy and precision of volumes dispensed from devices, laboratories must first understand how liquid delivery processes can fail and the effects of such failures before they can implement optimal LDQA programs.
The magnitude of risk caused by liquid delivery devices themselves is significant. Research shows that up to 30 percent of pipettes and other liquid delivery devices currently in service are not performing within expected tolerances at any given moment. The risk of non-performing liquid delivery devices is compounded by the ever smaller volumes typically handled in today’s laboratories. This means that volumes that are inaccurate by just a few microliters can have significant effects on results. For these reasons, error caused by handheld pipettes will be the focus of this inaugural article in the “Minimizing Liquid Delivery Risk” article series, and automated liquid handlers the focus of the next.
Consequences of Pipette Failure
In the best case scenario, using a pipette that is not performing accurately results in the need to retest samples or reevaluate data. While this does waste time, resources and money, the consequences are not as severe as when a malfunctioning pipette generates inaccurate test results used for treatment or when samples cannot be retested. This has a far greater impact with much higher costs of failure.
The worst case scenario is the failure to identify in a timely fashion a pipette’s performance as being out of tolerance, leading to continued use of the pipette, and consequent reporting of inaccurate data and inaccurate results. This is clearly unacceptable for life and health science laboratories. Failure not only requires costly and time-consuming remedial action, but also puts patients and research at risk. (This is one of the reasons why the FDA has embraced the concept of Process Analytical Technology, whereby quality assurance is actively built into a process to detect and correct potential problems as they arise.)
Fortunately, careful examination often shows evidence of the source of failure, and many of these causes are preventable. Understanding pipette failure and preventing recurrence may be the most cost effective means of reducing costs and risk while improving quality and compliance.
How Pipettes Fail
First, it is important that laboratories define device failure. During calibration, the liquid volumes dispensed by the pipette being tested are compared against a standard and the deviation from this standard is measured. Performance outside of acceptable limits is defined as failure.
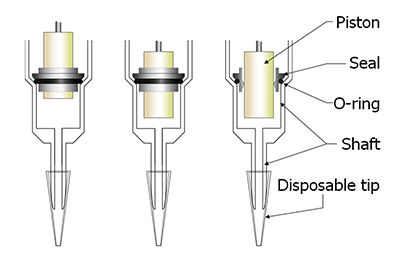
As today’s electronic pipettes are complex, relying on a number of internal components for proper function, damage is often not visible to the eye or evident by the feel of the pipette action. This is called a silent pipette failure. Silent mechanical failures can take many forms, from improper lubrication, to seal or o-ring leakage, damage to the shaft where it seals with the tip, corrosion of the piston and contamination by the materials being pipetted. These errors can be highly detrimental if operators unknowingly use malfunctioning pipettes in critical assays, diagnostic tests and experiments.
Figure 1. Major Points of Failure
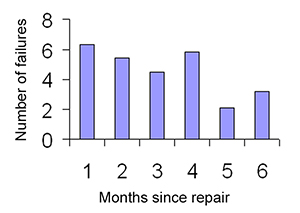
While pipette maintenance should be performed on a periodic schedule and can correct the abovementioned causes of mechanical failure, data collected in a laboratory where pipettes were heavily used showed that the time elapsed since a pipette’s last maintenance did not influence the probability of it failing in the next time period. Figure 2 shows the percentage of pipettes that failed each month for the six months between calibration intervals. There are two important conclusions to be drawn from this data. First, the failure rate is relatively constant: it does not increase every month as one might expect it to do. Second, in aggregate terms, approximately 27 percent of the monitored pipettes failed at some point during this six-month cycle. Even recent maintenance cannot guarantee that all pipettes will perform satisfactorily, and laboratories should expect some pipettes to fail during the time between calibrations.
Figure 2. Time to Failure
The data presented in this graph show a relatively constant failure rate as months elapse between calibration cycles. This means that even recent maintenance does not guarantee that all pipets will perform satisfactorily and that laboratories should expect some pipets to fail during the time between calibrations.
Even more alarming is that only 10 percent of pipette failures are due to normal wear factors such as frequency of use and time since last maintenance. On the other hand, ninety percent of failures are random and unpredictable, caused by incidents such as accidents or misuse. For example, piston corrosion or premature seal failure may result if an operator accidentally draws liquid into the body of the pipette. Also, if the operator lays the pipette down while some fluid still remains in the tip, the fluid can flow up inside the shaft and contaminate seals and rings.
Solution: Regular Calibration and Verifications of Pipette Performance
To offset the risk and impact of out of tolerance pipettes and to quickly identify those that are failing, regular calibration programs and verification checks must be implemented.
Critical to an effective calibration program is the frequency at which calibrations are conducted, and the optimal frequency depends on the following factors:
Mean Time Before Failure: The average rate at which failures occur can be expressed as Mean Time Before Failure (MTBF). As opposed to the failure rate represented in Figure 2, measuring the number of failures per unit of time, the MTBF measures the cumulative number of failures in a group of pipettes over a period of time to determine the average time elapsed between failures. Therefore, the MTBF and failure rate are inverses to one another: a high MTBF is based on a low failure rate. A high MTBF is desirable because it means that the chance of any given pipette having failed is small.
Using the MTBF, one can predict how long a pipette can be expected to maintain accuracy and precision. The MTBF for individual pipettes can vary significantly, depending on a number of factors. For example, a pipette used daily will fail more quickly than a pipette used less frequently. In addition, the delivery of gummy, chemically aggressive or corrosive samples will also reduce the MTBF.
One way to determine MTBF, is to track a group of pipettes until each one fails, determining how long it takes each pipette to fail. The mean of all the failure times is the MTBF for that specific group of pipettes.
The MTBF can also be determined mathematically, using the formula below:
t is the time since the last calibration;
% failed is the cumulative percentage of pipettes found to have failed since the last previous calibration.
In the data shown in Figure 2, a total of 27.3 percent of the pipettes failed on or before the six-month interval. Using the above equation for t=6 and %failed=27.3, the MTBF is calculated to be 18.8 months.
Target Reliability Level: Current best practices for pipette management are to establish target reliability levels at 95 percent or higher. This means that on recalibration or verification, at least 95 percent of the pipettes will be found to be operating within established tolerances, with only 5 percent generating incorrect results. When determining a desired target reliability level, factors such as assay precision, the impacts of failed pipettes on test results, legal defensibility of results and production batch release decisions are important. Compliance with regulatory guidelines may also be applicable.
Once the established target reliability level for a laboratory and the MTBF for the pipette population are determined, the following formula can be used to identify the optimal calibration frequency:
Cal_Interval is calibration frequency in years needed to achieve the target reliability level
MTBF is the mean time before failure in years
ln is the natural logarithm
TRL is the desired Target Reliability Level in percent
As an example, when a laboratory’s desired Target Reliability Level is 95 percent and the MTBF is two years, the calculated calibration interval is 0.103 years, or every 5.3 weeks.
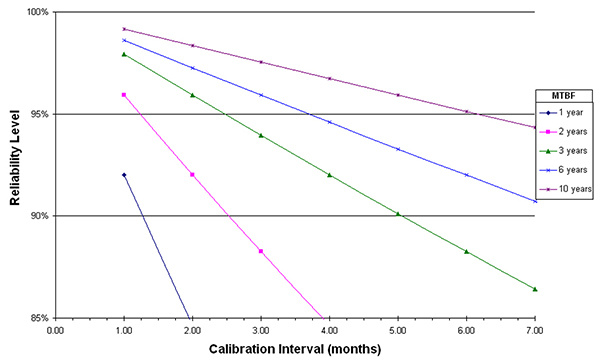
Figure 3. Reliability Model for Determining Optimal Calibration Frequency
Once the established target reliability level for a laboratory and the Mean Time Before Failure for the pipette population are determined, this figure can be used to identify the optimal calibration frequency.
In Figure 3, common MTBF figures and target reliability levels have been plotted, which laboratories can use to determine optimal calibration frequencies. Suppose that the required target reliability level is an industry best practice of 95 percent and the MTBF is two years. To determine the appropriate calibration frequency, follow the line indicating MTBF of two years in the graph until it meets the 95 percent level on the Y-axis. The corresponding point on the X-axis indicates the required calibration interval, which, in this case, is between five and six weeks. Therefore, checking these pipettes at least every five to six weeks should achieve the established pipette performance quality objective.
Quality Control Principles: Like all precision laboratory instruments, mechanical action pipettes should be subject to quality control principles. Just as is required for spectrophotometers and balances, pipettes should be calibrated on a regular basis to verify performance.
The more frequently pipette checks (calibration or verification) are performed, the sooner malfunctioning pipettes will be detected and taken out of service. Conversely, the longer a defective pipette remains in service, the greater the liability it presents.
Regulations: Regulations and standards published by organizations such as the International Organization for Standardization (ISO), the U.S. Food and Drug Administration (FDA), Clinical Laboratory Improvement Amendments (CLIA) and ASTM International provide minimum requirements with varying degrees of specificity that help ensure the quality of laboratory results. These form the groundwork upon which a laboratory should establish the frequency of pipette calibration as part of good quality control practices.
It is important to note that documentation is critical to developing and implementing a regular calibration program, as well as complying with regulations. If it is not documented, it did not occur in the eyes of regulatory bodies.
It should be noted that critical assays may require interim verification checks between calibration cycles, a procedure made feasible by easy to use, in-house calibration technologies. Indeed, the Center for Disease Control (CDC) specified in a 2005 training manual the necessity for “function checks” of pipettes before certain specific tests are performed. Many laboratories have also adopted interim checks of pipettes. This process is often used to ensure proper pipette performance in the following situations: 1) between calibration cycles to manage the risk of failure and reduce potential remedial actions; 2) before critical assays; 3) before using rare reagents or limited samples; and 4) to ensure that the production of standards is accurate to avoid downstream failures within a company that relies upon those standards in various operations.
Risk Reduction
In life and health science laboratories, producing data used to diagnose illness, treat patients and develop new drugs, uncertainty must be closely managed. The ubiquity of pipettes in laboratories coupled with the potential for failure make the propensity for error large. In order to build quality into laboratory results, the performance of pipettes must be verified at regular intervals. Simple steps including developing and implementing a regular calibration program, implementing an interim check and understanding pipette usage and failure can be taken to minimize this source of uncertainty and ensure data integrity.
Related Resources
Learn more by checking out our additional educational resources below.
Clinical Case Study
Keeping Plasma Safe: Haematologic Technologies Inc. Implements the Artel PCS for Quality Assurance